One of the treatments for POTS is an increase in fluid intake to increase blood volume to reduce the risk of hypotension and even tachycardia, as seen on the POTS page. For some POTS patients, it is hard to drink the recommended 2-3 liters of water a day or for others, this amount may not be enough to be effective. After conducting a literature review, no peer reviewed articles were found explicitly discussing IV hydration therapy and POTS. This is not surprising because literature on POTS in general is sparse. Many POTS patients have reported a substantial improvement in the quality of their life and a lessening of their POTS symptoms after receiving IV saline.
For infrequent IV saline use, some POTS patients visit emergency rooms or urgent care centers. One way to receive IV fluids on a consistent basis is through the use of a temporary PICC line. Another way patients receive IV fluids on a consistent and more permanent basis(versus a PICC line) is through the use of a port.

A port is a small medical device that is inserted beneath the skin. The device is surgically implanted under the skin in the upper chest area and a catheter connected to the port is inserted into a vein, typically in the neck area. The surgery is considered minor and is typically performed under conscious sedation and local anesthesia by a surgeon or interventional radiologist. The port itself has a septum which is a rubber material, where the Huber needles puncture for access the port. While under the skin, the port can be accessed to either inject substances(IV saline), or draw blood samples. Typically these needle sticks are less painful than typical needle sticks and allow for the veins in the arms to be spared.
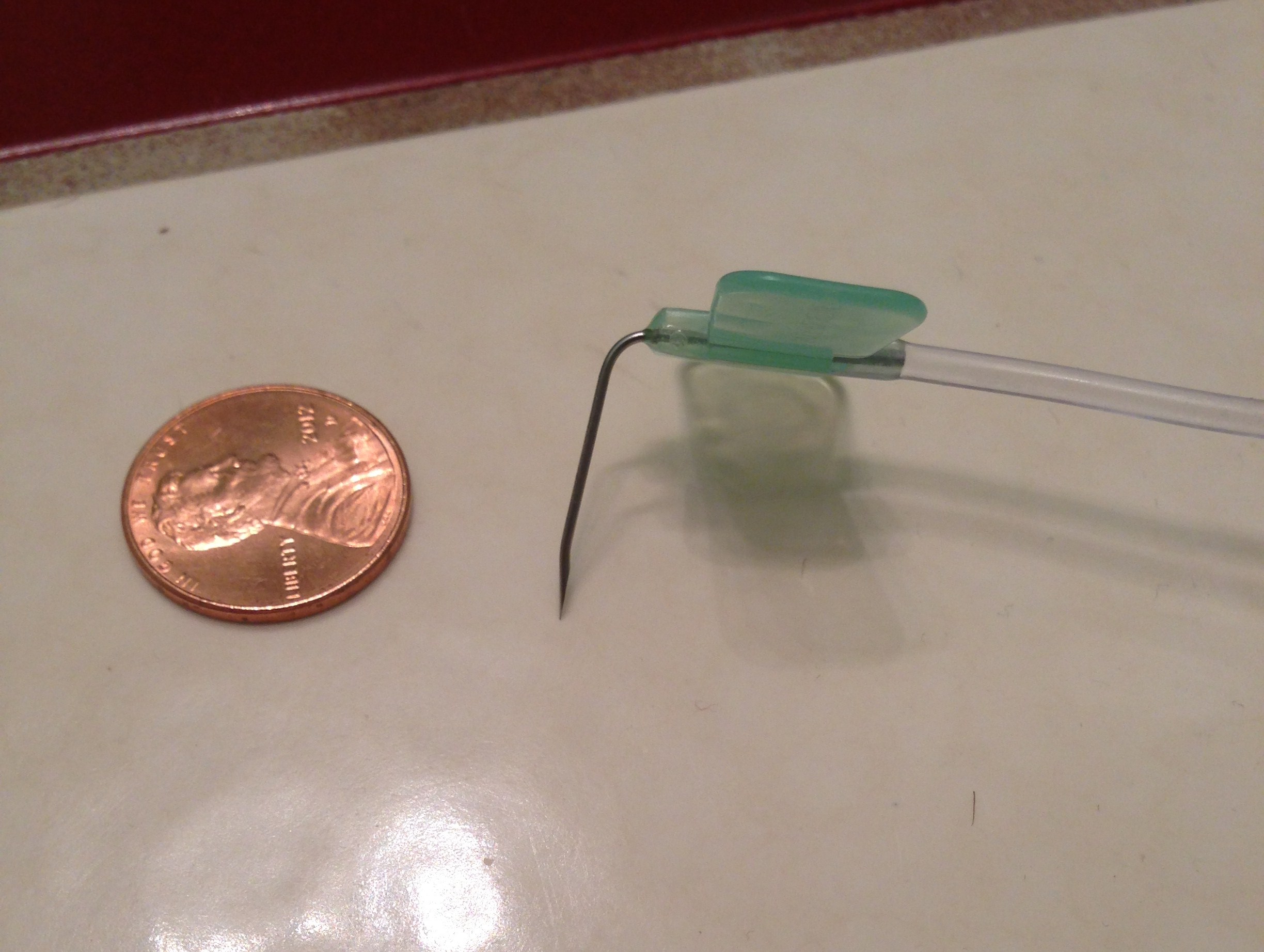
To administer IV saline, the port needs to be accessed by puncturing the overlying skin with a 90° Huber point needle. Proper protocol needs to be followed by a health professional or trained patient in order to access the port and prevent infections. The port can be left accessed for as long as required and can typically be left accessed for 5-7 days before a needle change. The port is covered in a dressing to protect the site from infection and to secure the needle in position. When no longer needed, the port can be removed in the operating room.
